The cardiac and smooth muscles are derived from the splanchnic mesoderm. The musculature of the body is derived from the mesoderm as described below:
Somatic mesoderm: Muscles of limbs and trunk
Branchial mesoderm: Muscles of head and neck
Splanchnic mesoderm: Cardiac and smooth muscles
However, there are certain exceptions and some muscles are ectoderm-derived. These include
Musculature of the iris (spincter and dilator pupillae)
Erector pili muscles in the skin
Myoepithelial cells of ducts of sweat glands
Q1327.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
The cardiogenic area is formed in which of the following structures?
Image not available for this question yet.
A) Extraembryonic mesoderm
B) Somatopleuric mesoderm
C) Splanchnopleuric mesoderm
D) Paraxial mesoderm
Correct Answer:C
Explanation:
The heart develops from angioblastic tissue in the splanchnopleuric mesoderm.
The heart develops from two endothelial heart tubes. These heart tubes are derived from the splanchnic layer of the lateral plate mesoderm also known as splanchnopleuric mesoderm.
Progenitor heart cells form a horseshoe-shaped cluster of cells cranial to the neural fold. This location from which the heart originates is known as the cardiogenic area.
The image below shows location of cardiogenic area during embryological development.
Q1328.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
Which of the following forms the trabeculated part of the right ventricle?
Image not available for this question yet.
A) Primitive ventricle
B) Distal 1/3 of bulbus cordis
C) Middle 1/3 of bulbus cordis
D) Proximal 1/3 of bulbus cordis
Correct Answer:D
Explanation:
The trabeculated part of the right ventricle is formed from the proximal 1/3rd of the bulbus cordis.
The heart tube begins to bend by day 23. This bending creates the cardiac loop. The fate of various structures formed as a result of this bending is as follows:
Given below are the heart tube and their derivatives:
Trabeculated part of Rt.ventr icleOutflow tract of Rt. and L t.ventriclesRoot and proxima l portions of aorta and pulmo nary artery
Trabeculated part of the Lt.v entricle
The common atrium that spli ts to Rt. and Lt.atrium
Q1329.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
Sinus venosus does not receive blood from which of the following veins?
Image not available for this question yet.
A) Vitelline vein
B) Umbilical vein
C) Common cardinal vein
D) Subcardinal vein
Correct Answer:D
Explanation:
The sinus venosus does not receive blood from the subcardinal veins. They are found in relation to the urogenital ridges and mainly drain the developing kidney.
Sinus venosus is the caudal-most part of the tubular heart and has right and left horns. Each horn of sinus venosus has 3 branches:
Vitelline vein receives blood from the yolk sac
Umbilical vein receives blood from the placenta
Common cardinal vein receives blood from the body wall
Q1330.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
A 2-year-old child was found to have an absence of coronary sinus associated with other cardiac defects. Failure in the development of which of the following structures will most likely lead to the given condition?
Image not available for this question yet.
A) Right umbilical vein
B) Right horn of sinus venosus
C) Left horn of sinus venosus
D) Left vitelline vein
Correct Answer:C
Explanation:
The coronary sinus develops from the left horn of the sinus venosus. Hence, its developmental failure will lead to defects of the coronary sinus.
Initially, the communication between the sinus venosus and the atrium is wide. Later, the entrance of the sinus venosus shifts to the right side due to the establishment of left-to-right shunts of blood.
The fate of sinus venosus and its branches near the heart is as follows:
Right horn of sinus venosus gets incorporated into the right atrium
Right umbilical vein: obliterates
Right common cardinal vein: Becomes part of the superior venacava
Right vitelline vein: Becomes the terminal part of inferior venacava
Left horn of sinus venosus reduces in size and becomes the coronary sinus
Left umbilical vein: obliterates
Left common cardinal vein: reduces the size and becomes the oblique vein of the left atrium
Left vitelline vein: obliterates
Q1331.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
A 40-year-old man had a CT scan to evaluate a lower respiratory tract infection. Incidentally, he was found to have a left-sided superior vena cava draining into the coronary sinus. The patient reported no cardiac symptoms. Failure of regression of which of the following structures during embryonic development leads to the given anatomical variation?
Image not available for this question yet.
A) Left anterior cardinal vein
B) Right anterior cardinal vein
C) Left common cardinal vein
D) Right posterior cardinal vein
Correct Answer:A
Explanation:
Persistent left-sided superior vena cava occurs due to failure of regression of the left anterior cardinal vein. It may drain either into the coronary sinus or the left atrium.
The formation of the vena cava system begins with the formation of anastomoses between the right and left venous channels. Formation of the major veins takes place as follows:
The proximal part of the right anterior cardinal vein along with the right common cardinal vein form the superior vena cava
The distal part of the right anterior cardinal vein between the junction with the subclavian vein and the junction with the transverse anastomosis becomes the right brachiocephalic vein
The distal part of the left anterior cardinal vein and the transverse anastomosis becomes the left brachiocephalic vein
The most cranial part of both the anterior cardinal veins above its junction with subclavian vein become the internal jugular vein
Q1332.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
88 The posterior cardinal vein contributes to the development of which of the following adult structures?
Image not available for this question yet.
A) Common iliac vein
B) Superior vena cava
C) Internal jugular vein
D) External jugular vein
Correct Answer:A
Explanation:
The posterior cardinal vein contributes to the development of the right common iliac vein. The common iliac veins develop as follows:
The right common iliac vein is derived from the most caudal portion of the right posterior cardinal vein.
The left common iliac vein develops from the anastomosis between the sacrocardinal veins.
Q1333.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
What is the location of the foramen secundum?
Image not available for this question yet.
A) Upper part of septum secundum
B) Lower part of septum primum
C) Upper part of septum primum
D) Lower part of septum secundum
Correct Answer:C
Explanation:
The foramen secundum (ostium secundum) is present at the upper part of the septum primum.
During fetal life, oxygenated blood reaches the right atrium from the placenta. This blood then reaches the left atrium through the gap between the atria. The initial gap is the foramen primum formed at the lower end of the septum primum.
Before the foramen primum is closed, another path has to be created for the flow of blood. This gap is the foramen secundum at the upper part of the septum primum.
Q1334.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
The limbus fossa ovalis is the remnant of
Image not available for this question yet.
A) Septum primum
B) Septum secundum
C) Both a and
D) None of the above
Correct Answer:B
Explanation:
The limbus fossa ovalis (also known as annulus ovalis) represents the remnant of the lower free edge of the septum secundum.
Fossa ovalis is an oval-shaped depression in the septal wall of the right atrium just above the opening of inferior vena cava. It marks the location of embryonic foramen ovale.
The floor of fossa ovalis is the remnant of septum primum.
The limbus of fossa ovalis is the prominent upper margin of the fossa ovalis and a remnant of the septum secundum.
Q1335.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
Which of the following structures does not contribute to the formation of the arch of the aorta?
Image not available for this question yet.
A) Left horn of aortic sac
B) Left 4th arch artery
C) Aortic sac
D) Left 2nd arch artery
Correct Answer:D
Explanation:
The left 2nd arch artery does not contribute towards the formation of the arch of the aorta. Arch of the aorta develops from the following:
Ventral part of the aortic sac
Left horn of the aortic sac
Left 4th arch artery
Q1336.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
Which of the following structures is derived from the right 4th aortic arch?
Image not available for this question yet.
A) Right common carotid artery
B) Right subclavian artery
C) Aortic arch
D) None as it regresses completely
Correct Answer:B
Explanation:
The proximal part of the right subclavian artery is derived from the right 4th aortic arch.
The distal segment of the right subclavian artery is derived from the right dorsal aorta and the 7th intersegmental artery.
The 4th aortic arch persists on both sides and forms different structures on either side:
Left side: Part of the arch of the aorta between the left common carotid and the left subclavian arteries
Right side: Proximal segment of the right subclavian artery
Q1337.
Anatomy
Medium
4m
Image ready
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
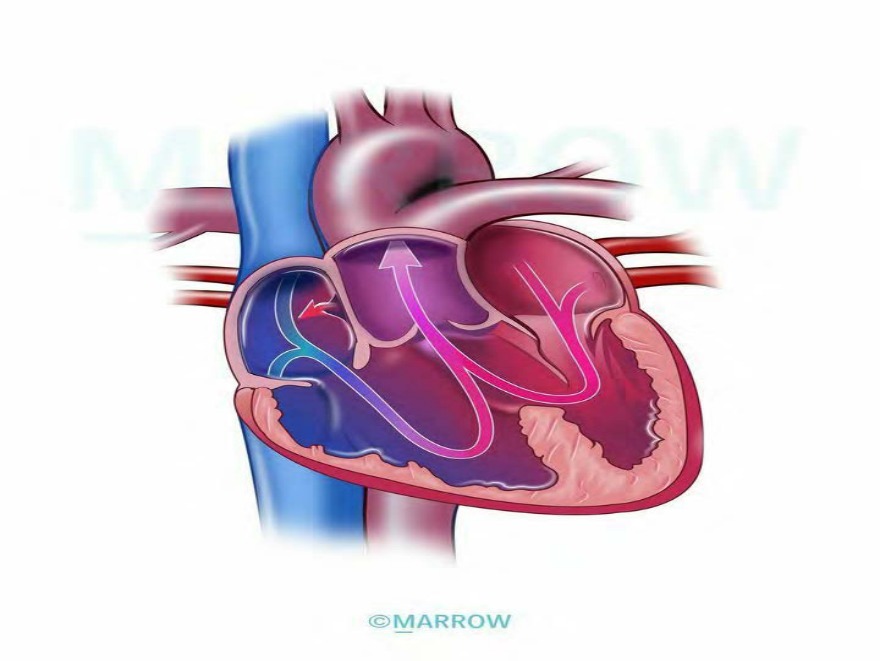
A newborn with persistent cyanosis was being evaluated. He was found to have a congenital heart disease that is schematically represented below. What is the most likely embryological defect causing this?
A) Abnormal spiraling of conotruncal septum
B) Failure in formation of conotruncal ridges
C) Anterior displacement of conotruncal septum
D) Total anomalous pulmonary venous connection
Correct Answer:B
Explanation:
The given scenario is suggestive of persistent (patent) truncus arteriosus. Failure in the formation
(absence) of conotruncal ridges leads to this condition.
The aortopulmonary septum is also known as the conotruncal septum. The formation of the aortopulmonary septum in the truncus arteriosus divides the outflow channel of the heart into the ventral aorta and the pulmonary trunk.
Persistent truncus arteriosus results when the conotruncal ridges fail to form. As the conotruncal ridges also participate in the formation of the interventricular septum, there will be a defective interventricular septum in this condition. The persistent truncus overrides both the ventricles and receives mixed blood from both sides.
Q1338.
Anatomy
Medium
4m
Image ready
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
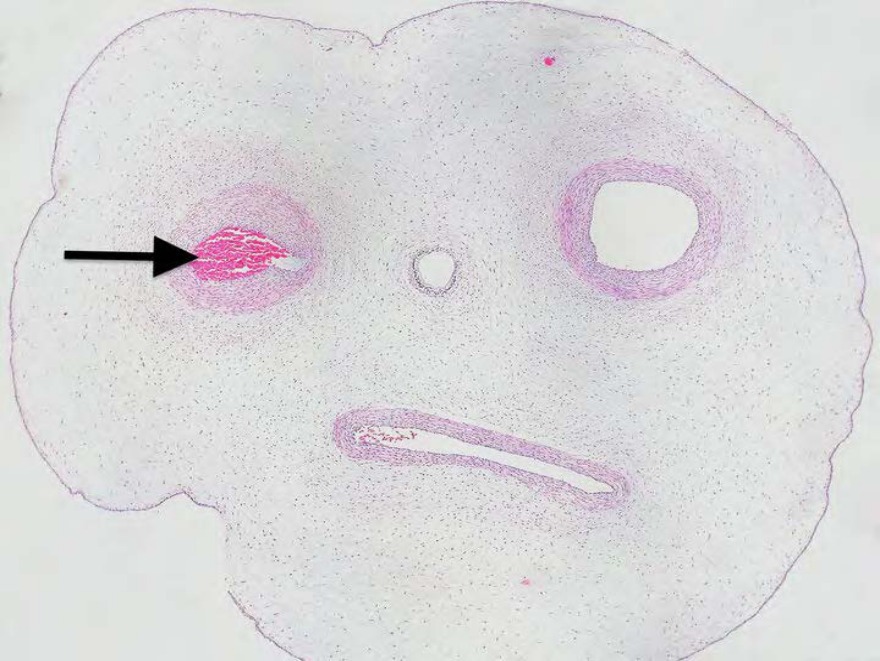
A cut section of the umbilical cord is given below. Which of the following is a remnant of the marked structure in an adult?
A) Ligamentum arteriosum
B) Ligamentum teres
C) Median umbilical ligament
D) Medial umbilical ligament
Correct Answer:D
Explanation:
The marked structure in the image is an umbilical artery. The medial umbilical ligament is the remnant of this structure.
The umbilical artery has the following fate:
Proximal parts persist as the superior vesical arteries
Distal parts get obliterated and form the medial umbilical ligaments
Given below are the embryological remnants at the umbilicus:
Embryological structur e
Left umbilical vein Umbilical arteries
Urachus
Remnant
ligamentum teres
medial umbilical ligament s
median umbilical ligamen t
Q1339.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
The heart starts to beat in the week of development.
Image not available for this question yet.
A) 2nd week
B) 4th week
C) 6th week
D) 10th week
Correct Answer:B
Explanation:
The heart starts to beat in the 4th week of development.
Q1340.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
The appearance of which of the following structures is regarded as the first sign of respiratory system development?
Image not available for this question yet.
A) Tracheoesophageal septum
B) Hypobranchial eminence
C) Primitive foregut
D) Laryngotracheal diverticulum
Correct Answer:D
Explanation:
The appearance of the laryngotracheal (respiratory) diverticulum is regarded as the first sign of respiratory system development. It appears in the ventral wall of the pharyngeal part of the
foregut.
The respiratory system is derived from 2 sources:
Endoderm of the foregut: The lining epithelium of the larynx, trachea, bronchi, bronchioles, and alveoli are derived from the endoderm.
Splanchnopleuric intraembryonic mesoderm: The cartilages, muscles, and connective tissue of the respiratory tract are derived from the splanchnopleuric intraembryonic mesoderm surrounding the foregut.
The image given below shows the development of the respiratory diverticulum.
Q1341.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
The larynx and the trachea develop from which of the following structures?
Image not available for this question yet.
A) Laryngotracheal tube
B) Laryngotracheal groove
C) Lung buds
D) Bronchial buds
Correct Answer:A
Explanation:
The larynx and trachea develop from the laryngotracheal tube.
The laryngotracheal (respiratory) diverticulum develops from the ventral wall of the pharyngeal part of the foregut.
The free caudal end of the respiratory diverticulum elongates downwards to enter the thorax, where it bifurcates to form the right and left bronchial buds or lung buds, which in turn further develops to form the bronchi and the lung parenchyma.
The part of the diverticulum cranial to the bifurcation is known as laryngotracheal tube, which further develops to form the larynx and trachea.
Q1342.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
Which of the following is the most common type of tracheoesophageal fistula (TEF)?
Image not available for this question yet.
A) Esophageal atresia with proximal TEF
B) Esophageal atresia with distal TEF
C) H type tracheoesophageal fistula
D) Proximal TEF with distal esophageal atresia
Correct Answer:B
Explanation:
The most common type of tracheoesophageal fistula (TEF) is esophageal atresia with distal TEF (also known as type C).
It occurs due to the defective formation of the tracheoesophageal septum. There is an abnormal connection (fistula) between the esophagus and the trachea. These defects occur in approximately 1/3000 births. The condition is commonly associated with esophageal atresia.
TEF can be grossly classified into 5 types, types A to E, as shown in the image below:
Q1343.
Anatomy
Medium
4m
Image missing
Topic: Cardiovascular and Respiratory SystemsSource: Internal
Explanation ready
A 5-day-old infant was admitted to the NICU as she was suffering from severe dyspnea and cyanosis. Chest X-ray revealed hypoplastic left lung and herniation of the intestines into the left thoracic cavity. Abnormality in which of the following structures during the embryonic development will most commonly lead to the given condition?
Image not available for this question yet.
A) Mesentery of the oesphagus
B) Pleuropericardial folds
C) Body wall
D) Pleuroperitoneal folds
Correct Answer:D
Explanation:
The given clinical scenario is suggestive of a congenital diaphragmatic hernia. It most commonly occurs due to failure of fusion of pleuroperitoneal folds during the development of the diaphragm.
The diaphragm develops from 4 mesodermal sources as follows:
Septum transversum becomes the anterior and medial part of the diaphragm including the central tendon
Pleuroperitoneal membranes (paired structures) become the dorsolateral parts of the diaphragm
Mesoderm of body wall from somites of cervical segments three to five (C3-5) contribute to the peripheral muscular part
Mesentery of the esophagus forms the crura of the diaphragm
Congenital diaphragmatic hernia results due to failure of various structures forming diaphragm to fuse. It occurs in 1/2000 births. The defect allows abdominal viscera to enter the pleural cavity. It is most frequently caused by the failure of one or both of the pleuroperitoneal membranes to fuse. Posterolateral defects (Bochdalek’s hernia) are the most common (85–90).
Q1344.
Anatomy
Medium
4m
Image missing
Topic: Alimentary, Hepatobiliary systems, Pancreas and SpleenSource: Internal
Explanation ready
Which of the following arteries supplies foregut derivatives of the digestive system?
Image not available for this question yet.
A) Celiac trunk
B) Superior mesenteric artery
C) Inferior mesenteric artery
D) Abdominal aorta
Correct Answer:A
Explanation:
The celiac trunk supplies the foregut derivatives of the digestive system. Arterial supply of the gut:
Foregut: Celiac trunk
Midgut: Superior mesenteric artery
Hindgut: Inferior mesenteric artery
Q1345.
Anatomy
Medium
4m
Image missing
Topic: Alimentary, Hepatobiliary systems, Pancreas and SpleenSource: Internal
Explanation ready
Which of the following structures give rise to the cecal bud?
Image not available for this question yet.
A) Pre-arterial segment of midgut loop
B) Post-arterial segment of midgut loop
C) Pre-arterial segment of hindgut loop
D) Post-arterial segment of hindgut loop
Correct Answer:B
Explanation:
The cecal bud arises as a diverticulum in the post-arterial segment of the midgut loop.
It enlarges and gives rise to the cecum and the appendix. The proximal part of the cecal bud grows rapidly to form the cecum. The distal part remains narrow and forms the appendix.
The midgut loop consists of:
Cranial limb - It forms
Jejunum
Upper part of the ileum
Caudal limb - It forms
Lower part of the ileum
Cecum
Appendix
Ascending colon
Proximal two-thirds of the transverse colon
Q1346.
Anatomy
Medium
4m
Image missing
Topic: Alimentary, Hepatobiliary systems, Pancreas and SpleenSource: Internal
Explanation ready
How much does the midgut rotate around the superior mesenteric artery?
Image not available for this question yet.
A) 270° counterclockwise
B) 180° counterclockwise
C) 270° clockwise
D) 180° clockwise
Correct Answer:A
Explanation:
The midgut normally undergoes a 270° counterclockwise rotation around the axis formed by the superior mesenteric artery.
The midgut forms a U-shaped loop (midgut loop) that herniates through the primitive umbilical ring into the extra-embryonic celom in the umbilicus. During the development of the intestines, the midgut loop rotates a total of 270° counter-clockwise around the superior mesenteric artery.
Around 90° rotation of the midgut occurs when returning from the physiological hernia in the umbilicus
The first part of the intestinal loop to retract from the umbilicus is the proximal portion of the jejunum
The last part of the intestinal loop to retract from the umbilicus is the cecal bud
The remaining 180° rotation occurs when the intestinal loops are in the abdominal cavity
Q1347.
Anatomy
Medium
4m
Image missing
Topic: Alimentary, Hepatobiliary systems, Pancreas and SpleenSource: Internal
Explanation ready
Which of the following will arise if there is the persistence of the vitellointestinal duct in a baby?
Image not available for this question yet.
A) Omphalocele
B) Gastroschisis
C) Meckel diverticulum
D) Urachus
Correct Answer:C
Explanation:
The persistence of the vitellointestinal duct gives rise to the Meckel diverticulum.
The primitive gut is connected to the definitive yolk sac through a narrow stalk-like communication known as the vitellointestinal duct. In about 2 of the population, a small section of the vitellointestinal duct persists to form an outpouching of the ileum called the Meckel diverticulum or ileal diverticulum.
Abnormalities arising due to incomplete obliteration of the vitellointestinal duct are given below:
Q1348.
Anatomy
Medium
4m
Image missing
Topic: Alimentary, Hepatobiliary systems, Pancreas and SpleenSource: Internal
Explanation ready
Which of the following structures does not develop from the endodermal cloaca?
Image not available for this question yet.
A) Rectum
B) Anal canal
C) Sigmoid colon
D) Urinary bladder
Correct Answer:C
Explanation:
The sigmoid colon does not develop from the endodermal cloaca.
The part of the hindgut that is present caudal to the attachment of the allantoic diverticulum is called the cloaca. Between the allantois and hindgut, a wedge of mesoderm, called the urorectal septum, grows. The urorectal septum divides the endodermal cloaca into two parts:
The primitive urogenital sinus in the anterior part develops into the urinary bladder, urethra, and lower part of the vagina (in females)
The primitive rectum in the posterior part develops into the lower part of the rectum and upper part of the anal canal.
The tip of the urorectal septum forms the perineal body.
Note: The rectum develops from both the hindgut (proximal part) and cloaca (distal part).
Q1349.
Anatomy
Medium
4m
Image missing
Topic: Alimentary, Hepatobiliary systems, Pancreas and SpleenSource: Internal
Explanation ready
A newborn boy had no passage of meconium for two days after birth. Examination revealed anal agenesis with perineal fistula. Which of the following is the most likely cause?
Image not available for this question yet.
A) Degeneration of the anal membrane
B) Failure of perforation of anal membrane
C) Incomplete separation of cloaca by urorectal septum
D) Failure of recanalization of the colon
Correct Answer:C
Explanation:
Incomplete separation of cloaca by the urorectal septum causes anal agenesis.
When the urorectal septum is formed, the cloacal membrane gets divided into urogenital membrane anteriorly and anal membrane posteriorly. The ectoderm in the region of the future anal opening is called proctodeum. The proctodeum invaginates and creates the anal pit. The anal membrane now separates the hindgut from the anal pit.
Formation of the anal canal takes place as follows:
The upper part of the anal canal is formed by the endodermal hindgut and the lower part by the ectodermal anal pit.
The anal membrane in between breaks around the 9th week and the anal canal becomes continuous.
The junction between the endodermal and the ectodermal region of the anal canal is marked by the pectinate line.
Q1350.
Anatomy
Medium
4m
Image ready
Topic: Alimentary, Hepatobiliary systems, Pancreas and SpleenSource: Internal
Explanation ready
A baby after delivery was found to have the following finding. The mother had no antenatal care history. Which of the following defects in the intrauterine life is the cause of this condition? 113
A) Failure of the intestinal loops to return from umbilicus
B) Defective closure of body wall in abdominal region
C) Defective closure of body wall in pelvic region
D) Defective closure of the vitellointestinal duct
Correct Answer:B
Explanation:
The given scenario is suggestive of gastroschisis. It is caused due to the failure of the body wall to close in the abdominal region during development.
Ventral wall defects include:
• Gastroschisis: The intestinal loops herniate through the defect in the abdominal wall. The defect usually lies to one side of the umbilicus (right side commonly). The loops of the bowel are not covered by amnion as they herniate through the abdominal wall directly into the amniotic cavity.
The affected bowel loops can be damaged by exposure to amniotic fluid.
Omphalocele: The bowel loops fail to return from the physiologic umbilical hernia. Since the umbilicus is covered by a reflection of the amnion, the omphalocele is also covered by amnion.
Bladder or cloacal exstrophy: Failure of the body wall to close in the pelvic region. Bladder exstrophy is less severe of the 2 and only the bladder is exposed in this condition. Cloacal exstrophy is more severe and both the bladder and rectum, which are derived from the cloaca, are exposed.
Ectopia cordis: Failure of the lateral body wall folds to close in the midline in the thoracic
region.
This results in the heart remaining outside the thoracic cavity.